Sleep and Orofacial pain
Sleep is an essential healing function for mind and body. Sleep and pain share a bidirectional relationship.
More here:
Pain can be both a cause and a consequence of sleep deficiency. This bidirectional relationship between sleep and pain has important implications for clinical management of patients, but also for chronic pain prevention and public health more broadly. Therefore, it is important for practitioners managing patients experiencing either sleep and/or pain issues to recognize and understand this complex association from a neurobiological perspective involving neuroanatomic and neurochemical processes. Accounting for the influence of pain on the various aspects of sleep and understanding its impact on various orofacial pain disorders assists in developing a prudent management approach (Klasser GD, Almoznino G, Fortuna G. Sleep and Orofacial Pain. Dent Clin North Am. 2018 Oct;62(4):629-656. doi: 10.1016/j.cden.2018.06.005. Epub 2018 Aug 14. PMID: 30189987; Lavigne GJ, Sessle BJ. The Neurobiology of Orofacial Pain and Sleep and Their Interactions. J Dent Res. 2016 Sep;95(10):1109-16. doi: 10.1177/0022034516648264. Epub 2016 May 6. PMID: 27154736.).
Machine learning has recently reported to highlight that sleep disorders significantly impact on the development of and persistence of chronic pain (Machine learning suggests sleep as a core factor in chronic pain Miettinen, Teemua,*; Mäntyselkä, Pekkab; Hagelberg, Norac; Mustola, Seppod; Kalso, Eijaa,e; Lötsch, Jörnf,g PAIN: January 2021 – Volume 162 – Issue 1 – p 109-123). They report that restorative sleep and significantly improve chronic pain levels (The effects of recovery sleep on pain perception: A systematic review.
Neuroscience & Biobehavioral Reviews ( IF 8.330 ) Pub Date : 2020-04-08 , DOI: 10.1016/j.neubiorev.2020.03.028 Cindy Stroemel-Scheder,Bernd Kundermann,Stefan Lautenbacher).
Sleep disorders impact on mental health and various conditions are known to impact on sleep including menopause and age.
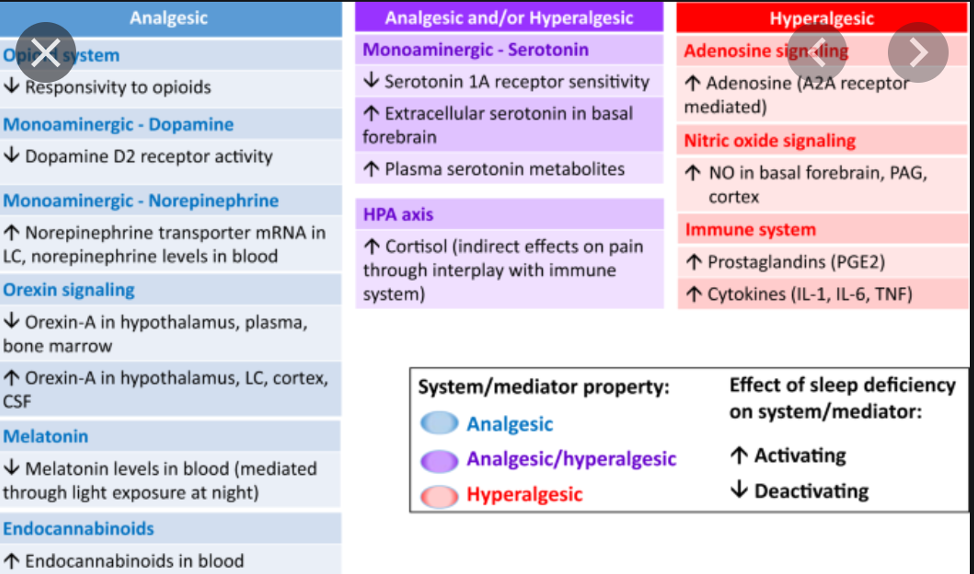
Sleep is fundamental to health and sleep disorders can often be a symptom of a disease; or also may be an indicator of a future disease such as depression. For those reasons, sleep assessment is an essential component of any health check. According to the majority of the studies, sleep deprivation produces hyperalgesic changes. Furthermore, sleep deprivation can counteract analgesic effects of pharmacological treatments involving opioidergic and serotoninergic mechanisms of action. The heterogeneity of the human data and the exclusive interest in rapid eye movement sleep deprivation in animals so far do not allow us to draw firm conclusions as to whether the hyperalgesic effects are due to the deprivation of specific sleep stages or whether they result from a generalized disruption of sleep continuity. The significance of opioidergic and serotoninergic processes as mediating mechanisms of the hyperalgesic changes produced by sleep deprivation are recognised (Stroemel-Scheder C, Kundermann B, Lautenbacher S. The effects of recovery sleep on pain perception: A systematic review. Neurosci Biobehav Rev. 2020;113:408-425. doi:10.1016/j.neubiorev.2020.03.028).
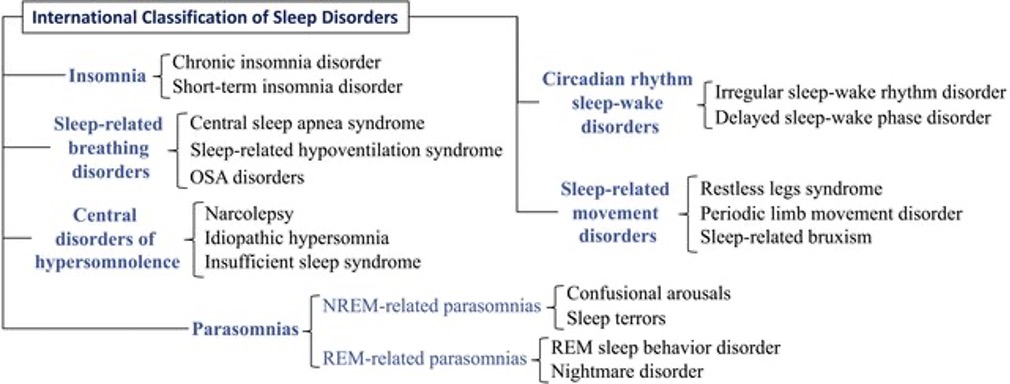
The International Classification of Sleep Disorders, 3rd ed., (ICSD-3) defines insomnia as difficulty falling asleep, difficulty staying asleep, or early awakening despite the opportunity for sleep that is associated with impaired daytime functioning and occurs at least three times per week for at least one month. Short-term, chronic, and other types of insomnia are the three major categories according to the ICSD-3. Insomnia can be acute (lasting up to three months) or chronic (lasting at least three months). Based on the severity of the disorder, all the criteria do not have to be met to begin therapy
Types of sleep disorders
Orofacial pain (OFP) is a complex, heterogeneous set of syndromes characterized by presentation of pain in the region of the face and oral cavity, arising from structures innervated by the trigeminal system. Chronic OFP (COFP; i.e., pain > 3 months) is a common problem, with an estimated UK prevalence of 7%.1 COFP is often very debilitating, dramatically affecting physical and psychological health, social function, and economic well-being of individuals.2-6 Broad symptomatic classifications of OFP distinguish between musculoskeletal pain (temporomandibular disorders; TMD) – comprising disorders of the temporomandibular joint (TMJ) and of the musculoskeletal structures (e.g., masticatory muscles), neuropathic syndromes – which include continuous (e.g., post-traumatic trigeminal neuropathy; PTTN) and episodic pain conditions (e.g., trigeminal neuralgia; TN) and neurovascular disorders – such as migraine and headache disorders.7
Orofacial pain can directly interfere with sleep, chronic pain is also recognised to interfere with sleep quality and quantity
More information below:
On the other hand, insufficient or inadequate sleep is know to contribute to increased pai intensity ad reduction of pain tolerance.
There are relatively few studies of the impact on sleep of orofacial pain disorders
Biopsychosocial factors and impact of chronic pain such as sleep quality can be used to phenotype the pain conditions and endotype the patients, in turn allowing for tailor-made treatment for each patient (Almoznino, Benoliel, Sharav, & Haviv, 2017; Bevers, Watts, Kishino, & Gatchel, 2016; Breeden & Rowe, 2017). Sleep is a vital component in individuals’ well-being, health and life, it can be affected by different factors, such as chronic pain (Karaman et al., 2014). Sleep disturbance is precipitated and perpetuated by chronic pain and are considered as one of the most common problems in these patients (Badawy, Law, & Palermo, 2019).
Results of a study by Karaman et al. (2014) indicated that around 41% of people with chronic pain experienced poor sleep quality. Moreover, a review conducted by Mills et al. (2019) stated that around half of the individuals living with chronic pain reported sleep deprivation due to their pain. This review also reported that there is a bidirectional relationship between sleep and pain, meaning patients with severe pain experience poorer sleep quality (Figure 1 ?). Therefore, as Campbell et al. (2013) concluded assessment and treatment of poor sleep can be beneficial in managing patients with chronic pain. Furthermore, Haviv et al. (2017) stated that assessment of sleep quality is vital in patients with OFP as it can negatively affect the health-related quality of life.
The evidence has shown that patients with chronic OFP including BMS, TN and PTNP reported poor sleep quality (Exposto et al., 2019). The prevalence of poor sleep in BMS patients is 80%, which is extremely high (Tan & Renton, 2020). A study by Haviv et al. (2017) reported the pain-related awakening in 50% of TN patients. Furthermore, Almoznino et al. (2017) stated that 41% of patients with PTNP experience pain-related awakening, this was 4 times greater than pain-related awakening in the healthy control group. This review also indicated that sleep deprivation is more significant in inferior alveolar nerve injury compared to lingual nerve injuries.
Therefore, in order to manage patients with OFP and sleep deprivation, dental health practitioners should evaluate and monitor OFP and sleep problems, and work in collaboration with other specialists including maxillofacial surgeons, psychiatrists and sleep medicine specialists if required (Almoznino et al., 2017). The use of instruments, such as the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepless Scale (ESS), Mini-sleep questionnaire (MSQ-BR) to evaluate the sleep quality is recommended (Dreweck et al., 2020). According to a systemic review conducted by Ali, Zolezzi, and Awaisu (2020), self-reported sleep instruments are the most practical methods to evaluate insomnia in clinical practice.
There is an emerging sub specialty in dentistry which focuses on screening and identifying risk factors in sleep disorders and their dental management of those patients with obstructive sleep apnoea (Frank Lobbezoo , Gilles J. Lavigne , Takafumi Kato , Fernanda R. de Almeida , Ghizlane Aarab. The face of Dental Sleep Medicine in the 21st century. A Review Journal of Oral Rehabilitation 16 August 2020).
Dentists have a fundamental role in early detection of potential OSA cases since they can use the methods identified in this review to perform an initial screening of the population.(Cecilia Rossi , DDS,Laura Templier , DDS,Manuel Miguez , DDS, MS, PhD,Javier De La Cruz , MDS, MS, MD-PhD,Adrián Curto , DDS, PhD,Alberto Albaladejo , DDS, PhD. Comparison of screening methods for obstructive sleep apnea in the context of dental clinics: A systematic review. JournalCRANIO® The Journal of Craniomandibular & Sleep Practice : 26 Sep 2020).
Another issue is that the medications used for managing pain also impact on sleep see below.
Assessment of sleep quality and quantity
The preliminary evaluation of sleep in primary care is often completed with a sleep questionnaire (also known as a sleep scale).
Sleep questionnaires are a very inexpensive and rapid test, and for these reasons, they are ideal for the first diagnostic test. They summarize in a quantitative way the (subjective) perception of the patient about his or her own quality of sleep. Mostly subjective, sleep questionnaires can be influenced by the same sources of bias and inaccuracy as any other such reports. However, their subjectivity does not necessarily render questionnaires inaccurate, as it has been demonstrated by several validation studies (Silvaetal.,2011;El-Sayed,2012;Firat etal.,2012; Luoetal.,2014; Patakaetal.,2014; Chai-Coetzeretal.,2015).
Many methods for sleep assessment have been developed and mainly focus on two methods:
- Sleep detection
- Sleep studies
- Self-assessment -Questionnaires
- An overview of sleep questionnaires is provided here
Triaging pain patients with sleep disorders is reported here.
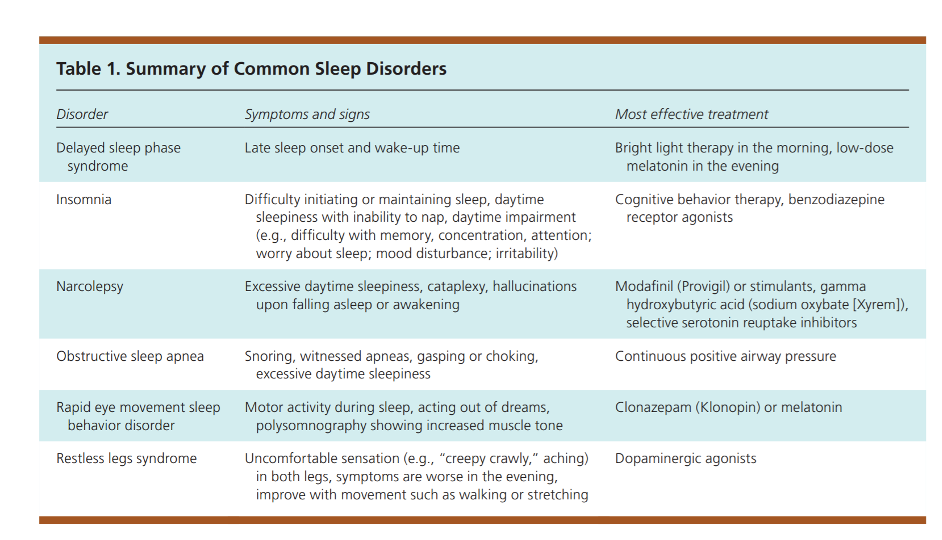
Management
Managing patients with sleep disorders will depend on many factors but primarily what type of disorder they have. The table below is by the AAFP
Also see the following links:
- Management of sleep disorders
- Management of OSA Lavigne Critical Review
- Management of chronic insomnia
- AAFP sleep disorders
Key words
OSA: Obstructive sleep apnea; PSG: Polysomnography; HST: Home sleep study; BMI: Body mass index; PPV: Positive predictive value; NPV: Negative predictive value; AHI: Apnea hypopnea index; RDI: Respiratory disturbance index; ODI: Oxygen desaturation index; PSQ: Pediatric Sleep Questionnaire; SRBD: Sleep-related breathing disorder; CSHQ: Children’s Sleep Habits Questionnaire; ESS: Epworth Sleepiness Scale; PSQI: Pittsburgh Sleep Quality Index
Danny Eckerts YouTube links
Dr Alex Nesbitt Neurologist/ Sleep Medicine Specialist